
Download this handy treat ladder guide from Blue Buffalo and Fear Free.
Download this handy treat ladder guide from Blue Buffalo and Fear Free.

Nail trims can be stressful for pets and owners alike. Set yourself and your pet up for success by downloading our nail trim handout!

Understanding Declaw Salvage Procedures
Until declaws are eliminated in the United States, you will most likely encounter declawed patients in your practice. With recent advancements in surgery, salvage procedures can help manage pain and improve limb function. Join one of the leading figures in declaw salvage surgery Nicole Martell-Moran, DVM, MPH, DABVP (Feline Practice), to learn about the procedures involved, how to find training, and how you can incorporate it into your practice.

Helping New Pet Owners Create a Fear-Free & Happy Life for Their Pet
New pet owners can be overwhelmed with all the information we want to provide them regarding the health and wellbeing of their pet. However, if a strong human-animal relationship built on trust and empathy is not established, the pet very well may not remain in the home. In this webinar, Kenneth M. Martin, DVM, DACVB, and Debbie Martin, CPDT-KA, KPA CTP, LVT, VTS (Behavior), will provide you with 5 tips to give new pet owners so they can start the relationship off on the right paw, facilitate a strong bond, and keep pets in the home and coming back to your veterinary clinic.
Brought to you by Vetoquinol
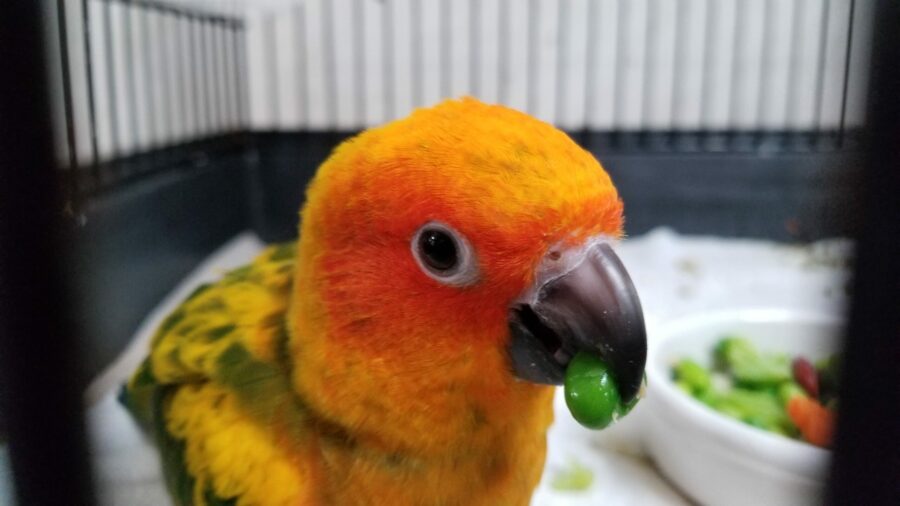
If birds love seeds and are engineered to eat them, doesn’t it follow that the bulk of a pet bird’s diet should be seeds? Absolutely not.
The nutritional needs of our birds’ counterparts in the wild may well be quite different from those of our pet birds, living in luxury in our homes. Also, the nutritional makeup of what they eat in the wild may be quite different from what we feed them in our homes. They’re living very different lives!
All-seed diets make most pet birds sick over time, because seeds deny them the nutrients they need for longer-term survival, add nutritional components that are excessive and unhealthy, and ultimately weaken them to the point where other diseases find it easy to take hold. The fact that pet birds can survive at all on such diets is a testament to the toughness of birds.
An all-seed diet contributes both directly (through malnutrition) and indirectly (by weakening the bird, making it easier for infectious disease to take hold) to a serious reduction in the possible life span of any pet bird – by half or more in many cases.
But birds know what’s good for themselves, right? After all, parrots are very intelligent. Well, so are you, but we bet that fact hasn’t stopped you from enjoying tasty treats that you know aren’t good for you. For birds, seeds are the equivalent of a greasy burger: junk food. And it’s that high-fat component that tends to get them in trouble. Too many pet birds (and people) are junk-food junkies.
Pelleted foods are a solid basis for a bird’s diet, but even pellets, wonderful as they are, probably need to be supplemented with vegetables, fruits, and other such “people food” as bread and pasta. Giving different foods in addition to pellets is a way to replicate the way most psittacines eat in the wild, consuming a wide variety of foods that vary seasonally.
This article was reviewed/edited by board-certified veterinary behaviorist Dr. Kenneth Martin and/or veterinary technician specialist in behavior Debbie Martin, LVT.
Excerpted from Birds For Dummies, 2nd ed., by Brian L. Speer, DVM, Kim Campbell Thornton and Gina Spadafori, Wiley, 2021.

The “fear center” and the “pain center” occupy adjacent areas of the brain. The thalamus is the area of the brain that registers pain, and on either side of the thalamus is the limbic system, which is responsible for emotions including fear, anxiety, and the sequelae of stress (FAS).
These two areas of the brain “talk” to each other and send signals back and forth. The thalamus sending signals to the limbic system is what causes your reaction to hitting your finger with a hammer. When this thalamic-limbic crosstalk happens in an animal in acute pain, the animal may lash out at the owner or veterinary staff.
So now consider an animal who is in pain and has been presented to you. If experiencing acute pain, the animal may lash out due to a combination of pain and FAS. If experiencing chronic pain, many of these pets act dull and disinterested. The owner may even comment that the pet just doesn’t socialize and lacks the energy and mobility that she used to demonstrate. Even worse is the animal who has chronic pain, say from osteoarthritis, and now has an acute injury on top of it. The distress in some of these animals is almost too much to bear.
It is easy for us to recognize and treat acute pain, but the diagnosis of chronic pain states can be difficult for a variety of reasons. It takes time to take a thorough history and perform a complete pain exam on dogs and cats. However, there are many resources available to make that task easier, including pet owner-friendly screening checklists for osteoarthritis (Cat, Dog) and expert tips for the OA exam (feline OA exam).
Even with successful diagnosis, the treatment of chronic pain can sometimes be difficult especially if your treatment is narrow in focus. But it is essential to make a timely diagnosis of chronic pain and provide effective analgesia to be successful in therapy. And it is also important that the owner understands your diagnosis, whether through education alone or with the help of radiographs and teaching tools (feline and canine chronic pain). The owner is an essential member of the pain treatment team, both in the evaluation of treatments over time but also in enlisting them in the day to day therapies that might be required.
My approach to the treatment of chronic pain in dogs, for example, is to build a pyramid of treatments, and on the base layer I start with an NSAID. The NSAID I use most commonly is Rimadyl® (carprofen), which I really like for its effects on both pain and inflammation. For many chronic OA cases, there are other factors that can influence the ability to manage both pain and disease progression, and they should all be looked at.
For example, consider the animal next. Is he overweight? One study showed that in an obese dog, losing only about 10 percent of body weight can significantly improve lameness1. In other words, weight loss for an overweight dog can amplify the pain relief achieved with an NSAID alone
What about exercise? Again, one human study showed that one-half hour of exercise 5 days a week for people with knee OA was the equivalent of – you guessed it: an NSAID! So now you have tripled your pain-relieving efforts by building a solid foundation of multi-modal therapies, upon which you can add other therapies as needed.
It is beyond the scope of this writing to discuss all possible treatments: medications, physical therapy, acupuncture, and so forth, but I encourage everyone to read or re-read the 2015 AAHA Pain Management Guidelines for a thorough review of all of the pain management options we have for both acute and chronic pain.
What does the future hold for us? The most exciting thing I have seen on the horizon is the introduction of anti-NGF monoclonal antibodies. NGF, or Nerve Growth Factor, is one of several major “players” in the transmission of pain via the nociceptors. The use of these monoclonal antibodies holds great promise to reduce the sensation of pain in our patients with osteoarthritis. More information about the action of anti-NGF monoclonal antibodies can be found at the New Science of OA Pain website.
IMPORTANT SAFETY INFORMATION FOR RIMADYL: As a class, NSAIDs may be associated with gastrointestinal, kidney and liver side effects. These are usually mild but may be serious. Pet owners should discontinue therapy and contact their veterinarian immediately if side effects occur. Evaluation for pre-existing conditions and regular monitoring are recommended for pets on any medication, including Rimadyl. Use with other NSAIDs or corticosteroids should be avoided.
See full Prescribing Information at:
https://www2.zoetisus.com/content/_assets/docs/Petcare/rimadyl-prescribing-information.pdf
Reference:
This article was reviewed/edited by board-certified veterinary behaviorist Dr. Kenneth Martin and/or veterinary technician specialist in behavior Debbie Martin, LVT.![]() Sponsored by our friends at Zoetis Petcare. ©2021 Zoetis Services LLC. All rights reserved RIM-00324
Sponsored by our friends at Zoetis Petcare. ©2021 Zoetis Services LLC. All rights reserved RIM-00324

These battered bonds are often related to behavior problems such as destruction to the home, inappropriate elimination, and aggression. In a 2013 study by Jennifer Y. Kwan and Melissa Bain, 65 percent of owners relinquished pets for behavior reasons. This study also supported the use of positive reinforcement, finding that use of punishment-based methods resulted in less satisfaction with a pet’s behavior, which can be damaging to the bond.1
The word “repair” means to restore by replacing a part or putting together what is torn or broken or to restore to a sound or healthy state. How can we repair a nearly broken human-animal bond? The role of a veterinary technician or assistant can be crucial in mending and strengthening this bond.
A skilled veterinary behavior professional should be able to demonstrate the prescribed behavioral therapy plans, coach the client through them, and be flexible with both pet and owner learning styles.2 In my practice, I describe my role as “case manager”: the person with whom each client is in contact with most frequently. It is my job to relay information clearly and effectively to the veterinarian and be sure that the entire behavior team (veterinarian, trainer, and owner) are working toward the common goal of restoring the bond.
Counseling aspects of behavioral medicine and marriage/family therapy have many commonalities.3 One of the most profound similarities is how change occurs in the context of treatment. In behavior medicine, our clients may come in with negative thoughts, anger, and fears associated with their pet. The veterinary technician or assistant’s role in the behavior team is to change the emotional experience of the pet along with that of the pet owner. When a family walks into our practice and their pet has been displaying owner-related aggression, my first questions are the following:
The client needs to express their concerns if treatment is going to be attempted. Behavioral therapy is essential, but the context and triggers of the problem are less important until people can form a more positive association with the pet. After the veterinarian discusses the behavioral diagnosis, I typically break down the information in a more down to earth fashion so the entire family can understand the mental concerns their pet has developed. In this way, the family can begin to relate to the pet and see things through their eyes, and this can jump-start the process of rebuilding the bond.
A second similarity to human-based therapy is the difficulties and barriers associated with clients.4 Most of our clients walk into the consultation room and expect to be told they did something wrong. They may be defensive, anxious, and closed off, reluctant to give a detailed behavioral history, which can impact treatment.
Sometimes clients are fearful about sharing a pet’s aggressive behaviors because they do not want to euthanize their pet. They feel as if they will be judged and forced to make an unwanted decision. One of my strongest skills as a behavior team member is gaining the trust of clients and building a strong rapport early on. I want each client and pet to have a wonderful experience with our clinic, but I also want to have a strong connection with that client, share empathy, and understand each issue from their perspective.
Clients may be at the end of their rope, but usually there is an inch of that rope left to work with. I think of the rope as the bond between owner and pet. Hang on to that tiny piece as it is still technically intact! Each client walks into the practice for a reason even if there is only a tiny strand of the bond remaining. If you can open them up, connect, and gain their trust, you can begin to reshape the negativity they feel toward their pet and repair the relationship.
One of the most important terms when repairing the human-animal bond is “empathy,” the ability to have a deep emotional understanding of another’s feelings and experiences.5 For veterinary behavior team members, this ability is crucial for success with any client or patient. They should be able to identify and empathize with the fear and anxiety the pet and client may be experiencing. This is the first step in modifying the behavior of both. Psychologist Marshall Rosenberg stated it best: “When we understand the needs that motivate ourselves and others’ behaviors, we have no enemies.” 6
I think this is important to recognize when working to rebuild or strengthen a human-animal bond. It is important for the client and veterinary behavior team to see things from the pet’s perspective. The client can then learn that the pet is not their enemy. The pet is not performing these behaviors to spite them. The pet is fearful, stressed, or anxious and may be trying to keep themselves safe. Being able to take a walk in someone else’s shoes, or paws, is a vital step in deepening the human-animal bond.
Mending the human-animal bond is not an easy task. It takes the expertise of a strong, educated, and skilled veterinary behavior team to even begin to reunite and mend the connection between client and pet. When working in a general practice, any sign that the human-animal bond is deteriorating between a client and patient should be brought to the team’s attention so the veterinarian can make a referral to a veterinary behavior practice.
As veterinary team members, we all want to save the lives of pets. This begins with keeping a strong bond between client and pet. Giving appropriate, science-based recommendations on training and behavioral therapy can be the first step in this process, starting with puppy and kitten visits. If we all work toward a common goal, we can make a difference.
References:
2-6. Shaw K. Julie, Martin Debbie. Canine and Feline Behavior for Veterinary Technicians and Nurses. 1st edition. John Wiley; 2015.
This article was reviewed/edited by board-certified veterinary behaviorist Dr. Kenneth Martin and/or veterinary technician specialist in behavior Debbie Martin, LVT.
Caring for Caregivers: The Three Areas Crucial to Mental Wellbeing
In this webinar presented by Natalie Marks, DVM, CVJ, you will learn about the variables that place veterinarians at high risk for mental health challenges and how to assess your own wellbeing. Dr. Marks will identify concerning signs in our own health and others as well as the three areas crucial to mental wellbeing: compassion satisfaction, compassion stress, and compassion fatigue. She will also provide realistic strategies to help veterinarians take care of themselves physically and mentally.
Brought to you by Virox Animal Health, Makers of Rescue

The Paw Project and Fear Free Together At Last!
The Paw Project’s beginning was rooted in helping relieve big cats from complications from being declawed. Thankfully, founder and director Dr. Jennifer Conrad saw the same need in domesticated felines. Don’t miss this opportunity to hear about her journey and her rebuttals against the common arguments in favor of elective feline onychectomy.

Fear Free Certified Practice Town Hall: Discontinuing Declaw Procedures
Following the announcement that Fear Free Certified Practices would be required to phase out elective feline onychectomies, we hosted a town hall with Fear Free founder Dr. Marty Becker, founder and director of The Paw Project Dr. Jennifer Conrad, pain management guru Dr. Michael Petty, and board-certified veterinary behaviorist Dr. Valarie Tynes. The “whys” behind this decision were shared and we wrapped up the hour with Q&A from the audience.